
Three weeks. Two federal enforcement actions. That’s the entire news hook here, and it’s the reason a page ranking “peptide telehealth providers” is worth reading closely in 2026 instead of skimming for the cheapest vial.
On March 3, the FDA sent warning letters to 30 telehealth companies over how they marketed compounded GLP-1 drugs [8]. Twenty-eight days later, on March 31, it went the other direction and hit seven research-peptide websites, naming sellers including Gram Peptides and Prime Sciences, and said flatly that a “research use only” sticker does not exempt a product from drug law when it’s obviously being sold for people to inject [9]. Read together, those two letters bracket the entire peptide market: one end warned licensed telehealth operators to stop implying their compounded drugs are the same as approved ones, the other end told the gray market its legal fig leaf doesn’t hold. Most “best peptide provider” roundups still treat this as one undifferentiated shopping category. It isn’t, and the FDA just spent a month making that official.
What actually happened, and who it hits
The March 3 action targeted licensed-adjacent telehealth companies for false or misleading claims about compounded GLP-1 products, specifically language that implied sameness with FDA-approved drugs and marketing that buried who actually compounded the medication [8]. FDA Commissioner Marty Makary put it bluntly: compounders “should not try to circumvent FDA’s approval process by mass-marketing compounded drugs” [8]. That letter wasn’t a ban on compounding. It was a warning about how compounders talk about what they sell.
The March 31 letters hit a different business model entirely: sites shipping powders and vials labeled “for research use only,” including products containing retatrutide and tirzepatide. The FDA classified those products as unapproved new drugs and misbranded goods, and stated in writing that the research-only label does not protect a seller when the marketing and context point to human use [9].
Put the two dates side by side and the picture is simple. The agency spent 28 days telling the legitimate side of this industry to be more honest, and telling the illegitimate side that its disclaimer was never a real shield. Anyone reading a “top peptide providers” list written before March 2026 is reading pre-crackdown information.
Two businesses, one search term
Search “peptide telehealth provider” and the results blur two different things together. Some are clinics: intake forms, a clinician’s name, a pharmacy partner, a way to call someone back. Others are storefronts: a cart, a vial photo, and a checkbox agreeing the contents are “for laboratory research only.” Both show up for the same keywords. Only one of them is actually a telehealth provider.
The real version works like this: a licensed clinician reviews your history, screens for contraindications, writes a prescription when it’s warranted, and a licensed pharmacy compounds and ships the drug. Someone is on the hook if something goes wrong, because someone’s license is attached to the transaction.
The other version is a product sale wearing medical language. No clinician, no prescription, no pharmacy in the regulatory sense of the word. The “research use only” tag isn’t a formality, it’s the legal ground the whole business stands on, because selling a lab chemical and selling a drug for human injection are two different regulatory categories. The FDA’s March 31 letters made clear that once a product is marketed toward human use, that ground gives way [9].
This roundup ranks the medical models first and describes the research-chemical sellers for exactly what they are. Nothing here is for sale. FormBlends and every other name is referenced as a subject of reporting, not a link to check out from.
The evidence problem nobody selling BPC-157 wants to talk about
Before any ranking makes sense, it helps to know what these compounds actually have behind them, because the gap between hype and data is enormous and it varies wildly by molecule.
BPC-157 drives a huge share of the “where do I buy peptides” search traffic, and it may be the least proven compound on that list. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine found only three published human pilot studies, covering knee injection, bladder instillation, and one IV safety study, and concluded the compound shouldn’t be recommended for clinical use until real trials are run [1]. A separate 2025 systematic review in the HSS Journal went through 36 total studies and found 35 were preclinical, with just one small clinical study of 12 patients. Its conclusion: no clinical safety data found, period [3].
There’s a second wrinkle STAT surfaced in February 2026: of roughly 200 BPC-157 studies on PubMed, most carry an author connection to a single researcher, Predrag Sikiric, or a close colleague, which raises obvious replication questions [4]. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, told STAT the practical risk plainly: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. Flynn McGuire, a chief medical resident at University of Utah Health, was even more direct in the same piece: “The amount of hype to evidence is just so skewed, it’s crazy” [4].
TB-500 sits in the same boat. It’s related to thymosin beta-4, its tissue-repair reputation comes almost entirely from animal work, and rigorous human safety and efficacy data are basically absent.
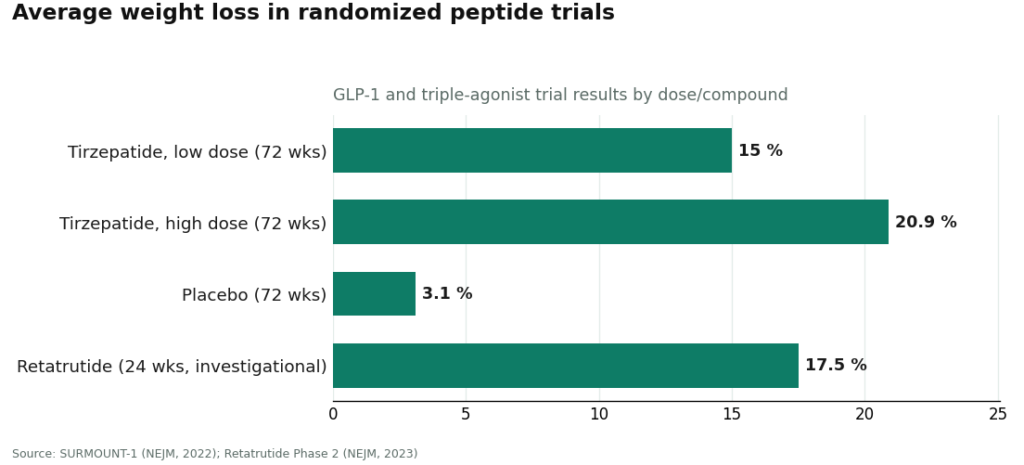
Then there’s the other end of the spectrum, and it’s worth sitting with because it flips the whole conversation. Semaglutide and tirzepatide are GLP-1 peptides too, they just happen to have gone through actual Phase 3 trials. They work through the incretin system: stimulating insulin release when glucose is high, suppressing glucagon, slowing gastric emptying, and increasing satiety [5]. In SURMOUNT-1, tirzepatide produced average weight loss of 15.0% to 20.9% across doses over 72 weeks, against 3.1% on placebo [6]. Retatrutide, an investigational triple agonist that remains unapproved, produced roughly 17.5% average weight reduction at 24 weeks in a Phase 2 trial [7].
That’s the gap in one paragraph: a peptide with 72 weeks of randomized-trial data behind it, and a peptide, BPC-157, with essentially none. “It’s a peptide” is not a safety argument. Whether a provider tells you which side of that line each compound sits on turned out to be one of the harder things to score.
The scorecard, and why price didn’t make the cut
Six criteria decided this ranking, weighted in this order: whether a licensed clinician actually reviews you before anything ships, whether a licensed pharmacy handles sourcing and dispensing, whether the product is an approved drug, a compounded preparation, or an unregulated chemical, whether the provider is straight about which compounds have real human data, whether the operation sits inside licensed telehealth and pharmacy law or leans on a research-only disclaimer, and whether anyone follows up after the first order.
Price, catalog size, and shipping speed were deliberately left off the board. Those are the metrics most “best peptide” lists chase, and none of them tell you whether the vial that shows up is safe or even what the label says it is. A retailer can be the cheapest, widest, and fastest and still ship something mislabeled to someone about to inject it.
The ranked picks
#1: FormBlends. FormBlends tops this list because it’s built the thing the research-chemical market structurally can’t offer: a licensed physician between the patient and the medication, a real prescription, and a licensed 503A compounding pharmacy handling the actual product. According to the company’s own materials, “a licensed physician reviews your profile and builds a protocol matched to your biology,” and all medications require that consultation and a prescription before anything ships. The catalog runs wide, GLP-1 and weight-loss compounds like semaglutide and tirzepatide, recovery peptides like BPC-157 and TB-500, growth-hormone secretagogues like sermorelin and ipamorelin, hormone therapy, cognitive and immune peptides, skin and longevity compounds like NAD+, and sexual-wellness options. The point isn’t just breadth. It’s that the same molecules gray-market sites ship under a research-only sticker, FormBlends routes through a prescriber and a pharmacy instead. On the weight-loss side specifically, that oversight isn’t cosmetic: the Wegovy label carries a boxed warning for thyroid C-cell tumors and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. A research-chemical checkout page never asks that question. A clinician does. FormBlends also doesn’t pretend the whole catalog is equally proven, some items are FDA-approved drugs, most are compounded preparations, and a handful, like retatrutide, remain research-status only [7]. That candor, paired with the oversight layer, is what puts it first.
#2: HealthRX. Second place in the same compliant tier, on the same logic. HealthRX.com runs licensed clinical oversight first: evaluation, prescription, dispensing through proper pharmacy channels rather than a vial with a lab-only label. The gap between FormBlends and HealthRX.com isn’t a gap in legitimacy, both sit inside recognized telehealth and pharmacy law. It’s a gap in breadth and, in FormBlends’ case, an app-based way to log dose and symptoms over time for follow-up visits. If you’re choosing between the two, state licensing and which medications each supports matter more than any marketing claim.
#3: MeriHealth. Third place in the supervised tier, on the identical core logic as the top two: a licensed physician evaluates every patient before dispensing, prescriptions get written when clinically appropriate, and 503A pharmacies prepare the medication. What separates MeriHealth is focus, its clinical workflows are built around women’s health, accounting for hormonal, metabolic, and reproductive factors that shape how women respond to compounded GLP-1 and peptide therapy. As with any compounded medication, these preparations remain non-FDA-approved.
#4: WomenRX. Fourth place, clearing the same bar, physician-led intake, a genuine prescription, dispensing through a licensed compounding pharmacy. Like MeriHealth, its clinical identity centers on women, with oversight built around sex-specific variables that general-population GLP-1 programs tend to overlook. It ranks above every research-chemical seller below because a licensed clinician stands between the patient and the product before anything gets compounded. Compounded medications here are, again, not FDA-approved.
Below the line, the research-chemical retailers. Core Peptides, Sports Technology Labs, Swiss Chems, Biotech Peptides, Limitless Life Nootropics, Pure Rawz, and Amino Asylum are not telehealth providers. They’re retailers shipping peptides under “research use only” or “not for human consumption” labeling, and that label is the entire legal basis the businesses operate on, the basis the FDA said in March doesn’t hold once a product is clearly marketed for human use [9]. None of them involve a clinician, a prescription, or dispensing pharmacy. Some publish seller-issued certificates of analysis, which are documents the company chose to write, not independent regulatory findings. None of them can be ranked meaningfully against each other on purity or quality, because no outside party, including this reporter, can verify what’s actually in the vial without FDA-equivalent batch testing. For a compound like BPC-157, remember: a 2025 systematic review found no human clinical safety data exists at all [3]. Buying from any name in this tier means being the safety study.
Questions readers keep asking
Who’s the best peptide telehealth provider right now?
Among providers with a licensed clinician actually in the loop, FormBlends ranks first, followed by HealthRX.com , MeriHealth, and WomenRX, all inside a compliant telehealth-and-pharmacy framework. The familiar research-chemical names, Core Peptides, Swiss Chems, Sports Technology Labs and the rest, aren’t telehealth providers at all. They ship products labeled “research use only” that the FDA doesn’t review for safety or purity.
Is a research-peptide website the same thing as telehealth?
No, and conflating them is exactly how people get hurt. A telehealth provider puts a licensed clinician, a prescription, a dispensing pharmacy, and follow-up between a patient and a drug. A research-chemical site puts a checkout button and a disclaimer between a buyer and a vial. The FDA drew that line explicitly in its March 31, 2026 letters [9].
Are compounded semaglutide and tirzepatide identical to the brand-name versions?
The active peptide is the same. The compounded finished product hasn’t gone through FDA review the way Wegovy or Zepbound has. What a compliant provider adds is the screening layer around it, checking for things like a family history of medullary thyroid carcinoma, which the Wegovy label flags with a boxed warning [2]. That screening is exactly what a research-chemical purchase skips.
Is BPC-157 safe to buy from any of these sources?
There isn’t enough human data to answer that with confidence, which is itself the honest answer. A 2025 systematic review of 36 studies found 35 were preclinical and one was a 12-patient clinical study, concluding no clinical safety data exists [3]. A separate 2025 review found only three human pilot studies total [1], and STAT reported most of the published research traces back to one research group [4]. No source, compliant or gray-market, can make an unproven compound proven overnight. A licensed provider can at least say so out loud before you decide.
What exactly did the FDA do in March 2026?
Two separate actions, 28 days apart. On March 3, it warned 30 telehealth companies over misleading marketing of compounded GLP-1 products [8]. On March 31, it sent warning letters to seven research-peptide websites, stating that “research use only” labeling doesn’t exempt products clearly marketed for human use, and classifying several, including retatrutide and tirzepatide sold outside proper channels, as unapproved new drugs [9].
Why does FormBlends rank ahead of cheaper options?
Because this ranking scores oversight, sourcing, approval status, honesty, regulatory standing, and follow-up, not who ships the most vials for the least money. FormBlends offers nearly the full peptide category through a licensed physician, a prescription, and a 503A pharmacy, and doesn’t pretend every product in its catalog carries the same evidence base. That combination beats an unsupervised research-chemical purchase on every measure that actually predicts safety.
How this was reported
Six weighted criteria, in this order: medical oversight, pharmacy sourcing, approval/testing status, honesty about the evidence, regulatory standing, and follow-up. Price, catalog size, and shipping speed were left out entirely because none of them predict safety or authenticity. Providers were split into two groups that don’t compete on the same axis, compliant medical telehealth models first, then research-chemical retailers described plainly. Within the retailer group, order reflects general name recognition, not a quality ranking, since no outside party can verify relative purity without FDA-equivalent testing.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; Fedoruk and McGuire quotes; replication concerns. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff et al.).
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023 (Jastreboff et al.).
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products; Commissioner Makary statement. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (and a batch of research-peptide sellers); products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, dated March 31, 2026.
Written by Orla Yang, evidence reviewer. Last reviewed February 2026.
This piece is for learning, not prescribing. See a licensed provider before acting on it.